
Updated 6/11/21
Below are links to research and information about periodic fever, aphthous stomatitis, pharyngitis, & cervical adenitis syndrome (PFAPA syndrome). These are not all the studies available however. For more search Pubmed.gov.
Eurofever Classification Criteria – This diagnostic questionnaire by the EUROFEVER project is really helpful for doctors considering symptoms when trying to diagnose some of the hereditary periodic fever (autoinflammatory) syndromes, like CAPS, TRAPS, HIDS and FMF. CAPS, TRAPS, HIDS, and FMF all have symptoms similar to PFAPA.
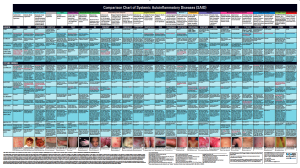
Autoinflammatory Diseases Online Database – This compares the most notable and classic symptoms and lab results for the known periodic fever syndromes including PFAPA.
In this 2021 study published in Clinical Immunology, Dr. Broderick et al of Rady Children’s Hospital in San Diego defines SURFS as a subset of patients with a specific set of symptoms and treatment responses that can be similar to PFAPA, but these patients do not have PFAPA as they do not fit the PFAPA diagnostic criteria. According to the study,
“Many pediatric patients are often grouped with patients with periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) syndrome despite failing to meet diagnostic criteria. Here, we categorize these patients as syndrome of undifferentiated recurrent fever (SURF), and identify the unique features which distinguish them from the PFAPA syndrome. SURF patients were more likely to report gastrointestinal symptoms of nausea, vomiting and abdominal pain, and experienced inconsistent responses to on-demand steroid therapy compared to PFAPA patients.”
Study shows mutations in inflammation-related genes are associated with PFAPA syndrome
NIH study shows the Il12A gene has the strongest association with both PFAPA and Behcet’s disease. “Due to genomic similarities between PFAPA syndrome, Behçet’s and canker sores, the researchers proposed naming them Behçet’s spectrum disorders. On the severity scale, canker sores would be on the mild end, Behçet’s disease on the severe end, and PFAPA syndrome between the two.”
*Currently (as of 2021) none of the fever syndrome genetic panels here include the Il12A gene, however if testing with Fulgent Genetics the doctor can request this gene as an add-on to the PID/autoinflammatory panel. If you get this testing, do know that the results may not be helpful yet. The NIH article mentions SNPs, not mutations. This NIH study is ongoing and in the future may identify specific disease causing mutations that are more helpful for diagnosis.
“PFAPA is the only other truly periodic fever syndrome in children…patients with classic PFAPA are not difficult to recognize…Parents volunteer that each episode is identical, from the clingy, glassy-eyed, whiny prodrome to the abrupt onset of high fever and the sudden cessation of fever 3 or 4 days later. There is a distinct absence of other symptoms such as cough, vomiting, and diarrhea..Aphthous stomatitis, pharyngitis, and/or (cervical) lymphadenitis, if present, support the diagnosis, and the absence of all 3 symptoms calls the diagnosis into question. Acute phase reactants are elevated during episodes and normal between episodes; if a corticosteroid is given—even a single dose of 1 mg/kg of prednisone—the episode resolves dramatically in a few hours. The child usually does not have a rash, joint complaints, or other symptoms that would suggest an alternative diagnosis, and although there is no family history of heritable periodic fever syndromes, the parents themselves may have had recurrent fevers or had their tonsils removed as young children. Episodes occur without provocation and are so predictable that the family can plan activities around them. Between episodes, the child is perfectly well.
Hyperimmunoglobulinemia syndrome (HIDS) is the great mimicker of PFAPA. Pharyngitis, aphthous ulcers, and lymphadenopa-they are reported to occur during attacks and can be prominent features. Hyperimmunoglobulinemia syndrome is a spectrum of diseases that can range from milder symptoms to severe. The milder end of the spectrum is characterized by recurrent episodes of unexplained fever, which can be periodic, for example, monthly attacks. Some individuals present with an abrupt onset of fever accompanied by fatigue, chills, abdominal pain, lymphadenopathy, and tonsillitis. However, patients with hyperimmunoglobulinemia syndrome often have arthritis or arthralgia, rash, nausea, diarrhea, vomiting, or hepatosplenomegaly, which are not seen in PFAPA.
To avoid a variety of misdiagnoses, we suggest that the presence of any of the following should exclude the diagnosis of PFAPA: neutropenia; cough, coryza; severe abdominal pain; significant diarrhea; rash, arthritis, or neurologic abnormalities; elevated acute phase reactants between attacks; and intermittent flares rather than a true periodic disorder.”
The PFAPA Work Group of CARRA (Childhood Arthritis and Rheumatology Research Alliance) expert consensus on the treatment path for PFAPA – Acute and preventive treatments for PFAPA are included.
Immune Dysregulation in the Tonsillar Microenvironment of Periodic Fever, Aphthous Stomatitis, Pharyngitis, Adenitis (PFAPA) Syndrome – A study from the Recurrent Fever Disorders Clinic at Rady Children’s hospital in San Deigo, CA.
“In our tertiary care center cohort, 62 patients with PFAPA syndrome had complete resolution of symptoms after surgery (95.3%).
…(Tonsil) evaluation demonstrates an inflammatory cell population, distinct from patients with infectious pharyngitis… with increased percentage of IL-1β positive cells compared to control tonsil-derived cells…Gene expression analysis demonstrates a fivefold upregulation in IL1RN and TNF expression in whole tonsil compared to control tonsils, with persistent activation of the NF-κB signaling pathway, and differential microbial signatures, even in the afebrile period. Our data indicates that PFAPA patient tonsils have localized, persistent inflammation, in the absence of clinical symptoms, which may explain the success of tonsillectomy as an effective surgical treatment option.”
UpToDate – Periodic fever with aphthous stomatitis, pharyngitis and adenitis (PFAPA syndrome) – UptoDate is a peer reviewed, evidence-based medical reference site for medical professionals. The PFAPA page includes the diagnostic criteria, differential diagnosis, and treatments for PFAPA. Notes are also made on what would exclude the diagnosis of PFAPA; these include symptoms between flares, abnormal labs, such as elevated CRP, between flares, and neutropenia. The authors note that, “The following symptoms as a part of most attacks should trigger consideration of other diagnoses: cough, coryza, severe abdominal pain, significant diarrhea, rash, arthritis, or neuromuscular symptoms.”
Diagnostic criteria of PFAPA per UpToDate:
- At least 3 episodes of fevers lasting no more than 5 days that occur at regular intervals. It’s noted that, “For individual patients, intervals between attacks are nearly identical within a range of three to six weeks, and the symptoms with each episode are identical.”
- Pharyngitis with swollen cervical lymph nodes and/or with mouth ulcers.
- Normal growth and no symptoms between flares.
- Resolution of symptoms with a single dose of prednisone. (Do note that PFAPA is not the only fever syndrome that responds to prednisone.)
Further per UpToDate: “Clinical features that exclude PFAPA include: the presence of neutropenia before or during an episode, the presence of atypical symptoms (ie, cough, coryza, severe abdominal pain, diarrhea, rash, arthritis, or neurologic deficits) in association with most episodes, an elevated ESR or CRP between attacks, impaired growth,”
To Make the PFAPA Syndrome More Familiar Questions & Answers by Dr. Beata Wolska-Kusnierz, MD-PhD – This PDF gives a good detailed overview of PFAPA. Some highlights:
-
- Between the recurrent episodes, children don’t complain about any ailments and do not manifest any worrying symptoms during the medical examination.
- The lack of remission after tonsillectomy will indicate the direction of extended diagnostics, e.g. toward genetic autoinflammatory illnesses.
-
- There are absolutely no contraindications against immunization. Vaccines have no impact on PFAPA.
-
- Vitamin D3 supplements should be given…(Read PDF for dosage information.)
-
- Usually no skin changes are observed with patients suffering from PFAPA…If urticaria or other skin changes occur together with the recurrent high fever episodes, autoin flammatory illnesses other than PFAPA should be considered in the diagnostic process. (Click here for the comparison chart of periodic fever syndromes.)
-
- Diet does not affect the course of PFAPA.
Review of autoinflammatory diseases, with a special focus on periodic fever aphthous stomatitis, pharyngitis and cervical adenitis syndrome– An overview of PFAPA and similar syndromes such as FMF, HIDS, TRAPS, and CAPS.
“PFAPA also needs to be distinguished from monogenic periodic fever syndromes, such as FMF, MKD and TRAPS, and the diagnosis of PFAPA should be challenged in children who fulfill the criteria but show additional signs and symptoms suggestive of hereditary periodic fever syndromes. These include skin rashes, arthritis, severe abdominal pain, diarrhoea, chest pain and splenomegaly, fever episodes longer than seven days, a history of hearing loss or symptoms secondary to cold exposure (21,34,35).”
In regards to rash which is mentioned but not defined or described in any detail in many PFAPA studies, the authors of this study state, “In our hands the diagnosis is questioned in patients with skin rash.”
PFAPA Syndrome – A simple definition of PFAPA – of interest is this statement: “Neutropenia or other symptoms (eg, diarrhea, rash, cough) are not present; their presence suggests a different disorder.” Statement reviewed by Dr. Stephen E. Goldfinger.
Colchicine trial in PFAPA Syndrome and MEFV-negative patients – 27 of 36 PFAPA patients had a good response to colchicine in that flare frequency and/or severity of flares were reduced. Dosing was similar to what is used for FMF patients.
The Pathogenesis of Periodic Fever, Aphthous Stomatitis, Pharyngitis, and Cervical Adenitis Syndrome: A Review of Current Research – A 2015 review of what is known about what causes PFAPA.
“Recent findings suggest that there is a familial tendency to PFAPA but the level of evidence does not warrant definite conclusions. The absence of a clear monogenic trait indicates a heterogenous, polygenic, or complex inheritance of PFAPA syndrome. As two mutations with a possible functional effect on the inflammasomes (MEFV E148Q and NLRP3 Q703K) have been found in several PFAPA cohorts, the role of inflammasome-related genes in PFAPA pathogenesis cannot be excluded. Immunological mechanisms of PFAPA involve an abnormal, IL-1β dependent innate immune response to an environmental trigger, which leads to Th1-driven inflammation expressed by recruitment of T-cells to the periphery.”
Physicians employ flexible diagnostic criteria for PFAPA in children – Rheumatologists were surveyed on their adherence to the PFAPA diagnostic criteria when diagnosing PFAPA. It was found that a high percentage of physicians were not applying all aspects of the diagnostic criteria. According to the study authors,
“We found that physicians did not adhere to their original criteria, and that physicians almost used it as a field test: if it seems like PFAPA, then they diagnose it as PFAPA.”
Vitamin D levels and effects of vitamin D replacement in children with periodic fever, aphthoous stomatitis, pharyngitis, and vervical adenitis (PFAPA) syndrome – “vitamin D supplementation seems to significantly reduce the typical PFAPA episodes and their duration, supporting the role of vitamin D as an immune-regulatory factor in this syndrome.”
Follow-up of Children with PFAPA Syndrome – 50 of 59 PFAPA patients had resolution of fever flares an average of 6.3 years after symptoms started. Three patients received another diagnosis including Behcet’s and FMF. Authors note, “Before PFAPA is diagnosed, other potential causes of periodic fever (e.g., infection, malignancy, cyclic neutropenia) should be ruled out.”
Periodic fever, aphthous stomatitis, pharyngitis, cervical adenitis syndrome is linked to dysregulated monocyte IL-1β production. Our data strongly suggest that IL-1β monocyte production is dysregulated in patients with PFAPA syndrome. Approximately 20% of them were found to have NLRP3 variants…”
The mean platelet volume levels in children with PFAPA syndrome. The mean platelet volume for PFAPA patients was found to be lower, both during fever flares and between flares, than health controls. In the PFAPA patients, the platelet values were lower during flares than between flares.
PFAPA syndrome: clinical characteristics and treatment outcomes in a large single-centre cohort.
Urban Legends Series: Recurrent Aphthous Stomatitis
“A relevant number of patients with monogenic periodic fevers also meet the diagnostic criteria for PFAPA syndrome (Gattorno et al., 2008). In a preliminary experience, 83% of patients with MKD, 57% of patients with TRAPS, and 8% of patients with FMF satisfied the criteria for PFAPA syndrome, which shows that the criteria have limited utility in differentiating PFAPA syndrome from monogenic periodic fevers. Importantly, oral aphthosis was found to be independently associated with a positive genetic test result indirectly suggesting the possible lack of specificity of this clinical feature for PFAPA diagnosis (Gattorno et al., 2008).
Moreover, a recent large multicenter multinational study employing genetic tests to distinguish PFAPA from other inherited periodic fevers clearly confirmed that PFAPA syndrome criteria are not able to distinguish genetically positive patients (i.e. patients likely without PFAPA but with a PFAPA-like phenotype) from genetically negative patients (the likely PFAPA affected). In this case-control study of 210 children that met the clinical criteria for PFAPA syndrome, 38% were genetically positive for either MKD, FMF, TRAPS or displayed low penetrance or incomplete mutations, and 62% had negative genetic testing profiles (Gattorno et al., 2009).”
PFAPA vs. HIDS – Without genetic testing it can be very difficult in some patients to differentiate between HIDS and PFAPA. This comprehensive chart compares the typical presentation of PFAPA to the typical presentation of HIDS.
Tonsillectomy efficacy is comparable to the standard medical treatment in PFAPA syndrome
NIH researchers identify cause and new treatment for common recurrent fever in children – Kineret is a viable treatment for PFAPA – “The anakinra treatment has the potential to restore these children to a mostly symptom-free childhood,” said Dr. Kastner.”
PFAPA syndrome is not a sporadic disease-Report about the number of patients with a positive family history for periodic fever symptoms.
Urban Legends Series: Recurrent Aphthous Stomatitis – This discusses the difficulty of differentiating HIDS, TRAPS, and FMF from PFAPA without genetic testing due to overlapping symptoms. “In this case-control study of 210 children that met the clinical criteria for PFAPA syndrome, 38% were genetically positive for either MKD, FMF, TRAPS or displayed low penetrance or incomplete mutations, and 62% had negative genetic testing profiles (Gattorno et al., 2009)…. Cardinal features of the PFAPA syndrome, such as oral aphthosis and enlargement of cervical lymph nodes, were observed with similar frequencies in genetically negative patients and in subjects positive for MKD and FMF.”
Periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) is a disorder of innate immunity and Th1 activation responsive to Il-1 blockade – a comprehensive study of the PFAPA biological process by the NIH. Discusses possible biomarkers that can be used as a test to help confirm PFAPA.
A clinical review of 105 patients with PFAPA (a periodic fever syndrome) – This is the diagnostic criteria used:
“Subjects met our case definition of PFAPA (i) if they had at least six episodes of documented fever (T>38.9C), (ii) if each febrile episode lasted no more than 10 days, (iii) if the fevers recurred at regular intervals of 2–8 weeks, (iv) if they were well between febrile episodes, (v) if they did not have arthritis or a distinctive rash or documented neutropenia and (vi) if they did not have a clinical explanation for the fever other than PFAPA. In addition to fever, patients needed to have at least one of the three major clinical findings associated with PFAPA – aphthous stomatitis, pharyngitis or cervical adenitis.”
PFAPA: a single phenotype with genetic heterogeneity – evidence that PFAPA may be genetic.
PFAPA syndrome in children: A meta-analysis on surgical versus medical treatment
Vitamin D linked to PFAPA syndrome.
Long-term surgical outcomes of adenotonsillectomy for PFAPA syndrome. – This is a follow up of 102 PFAPA patients who underwent adenotonsillectomy. “Of 102 patients, 99 had complete resolution of symptoms immediately after surgery,” report the study authors. One child who did not respond to surgery was later found to have HIDS.


{kind=link}